A guide to prescribing errors in healthcare
Few scenarios trouble health professionals more than prescribing the wrong medication and potentially causing a patient harm. An estimated 237 million medication errors occur each year in the NHS in England, with prescribing accounting for approximately 21% of these.¹
Most of these errors are minor but some have serious outcomes including death. It is therefore unsurprising that this issue is a major patient safety concern across healthcare settings.
Please complete the form at the bottom of this article to request a complimentary trial of MedicinesComplete.

Health professionals frequently work under significant pressures, including high patient volumes, staff shortages, and constraints on time, all of which can increase the risk of errors.²
The NHS Patient Strategy highlighted that high workload and frequent interruptions are contributors to medication errors.³
Education and training about errors and their causes is an important preventive strategy but health professionals often say that not enough time is dedicated to this.²
In the NHS, medication errors are generally considered as Patient Safety Incidents (PSIs). They may occur in the process of prescribing, preparing, dispensing, administering, monitoring, or providing advice on medicines.⁴ ⁵
Prescribing errors refer more specifically to “a failure in the prescribing process that leads to, or has the potential to lead to, patient harm”.⁵
Prescribing errors primarily occur during the selection and ordering of medicines. In contrast, dispensing errors take place during preparation and supply, while administration errors happen when the medicine is given to the patient. To ensure patient safety, health professionals should be aware that errors can occur at any of these steps in patient care.
Common types of prescribing error
Prescribing errors are a frequent and often preventable source of patient harm. While many result in ‘near misses’ or minor adverse effects, some can have serious consequences, especially when high-risk medicines are involved or they occur during transitions of care.
It is vital that health professionals are aware of the main types of prescribing error. Although categories may overlap, several types are consistently identified across healthcare settings.
Recent articles in the Pharmaceutical Journal have drawn attention to some of the specific challenges of medication errors.⁶ ⁷ ⁸ These include: a ‘top ten’ prescribing errors responsible for severe harm; high-risk medicines; and ‘look-alike sound-alike’ errors. Some examples of prescribing errors are highlighted below:
- Critical medicines not prescribed or supplied on time: This involves unintentional omissions or delays with medicines that are essential for maintaining therapeutic effect or preventing deterioration. These errors commonly occur during transitions of care, such as admission, transfer, or discharge, when communication gaps or incomplete medicines reconciliation lead to medicines being missed. For some medicines even short delays in administration can result in significant harm.⁶ ⁹
- Incorrect dosing: These errors are extremely common and ‘high-risk’ medicines are frequently involved.⁷ High-risk medicines include opioids, hypoglycaemics, anticoagulants, cytotoxic drugs, non-steroidal anti-inflammatory drugs (NSAIDs), antiplatelets, diuretics, corticosteroids, oxygen, and cardiac glycosides. Error rates with these drugs are not necessarily higher than with other medicines, but when problems occur the consequences can be more significant. A dosing error usually leads to a patient taking too much or too little of a medicine with the potential for drug toxicity or sub-therapeutic dosing respectively. For example, failure to consider a patient’s opioid-naive status or previous analgesic use when prescribing an opioid can lead to oversedation and respiratory depression. Safe opioid prescribing requires careful dose titration and regular review to ensure the chosen regimen remains appropriate.⁶
- Calculation errors: Mistakes when calculating or converting drug doses are also common. These errors can also occur with opioids, for example when dose equivalence is miscalculated when changing from one opioid to another. Another example can arise with loading doses of certain medicines, such as phenytoin, when it is necessary to rapidly achieve therapeutic blood levels. These calculations can be complex with multiple steps involved leading to prescribing errors.
- Wrong product, formulation, or strength: These errors often occur when a medicine is being dispensed or administered, but they can also occur at the prescribing stage. ‘Look-alike, sound-alike’ errors happen with medicines that have similar names, packaging, or multiple formulations.⁸ Selection of the wrong medicine from the drop-down menu in electronic prescribing systems is a known cause of serious harm. These systems have been widely implemented in the expectation that they would reduce medication errors, but they also make it easy to select the wrong drug.⁸ The wide range of insulin products available is a common source of confusion when prescribing, where mix-ups between rapid-acting, intermediate, or long-acting preparations lead to choosing the wrong preparation.⁶
- Inappropriate prescribing: Prescribing errors include irrational and inappropriate prescribing. For example, prescribing a medicine where there is a contra-indication, such as the use of a NSAID in patients with renal or cardiovascular risk factors. Failure to prescribe, such as not ensuring the use of a gastroprotective agent alongside NSAIDs or dual antiplatelet therapy can lead to avoidable adverse events.⁶
- Failure to monitor therapy: Some medicines require regular laboratory monitoring to ensure safe and effective use. Errors occur when these tests are not arranged, performed, or reviewed, resulting in undetected toxicity or treatment failure. Medicines such as ACE inhibitors, lithium, digoxin, and methotrexate require regular monitoring, and lapses can have serious consequences.⁶ With anticoagulants, missing essential INR checks, or failing to adjust therapy based on results, can lead to preventable complications. These errors often arise when it is unclear who is responsible, when there are poor follow-up systems, or when there is the assumption that monitoring is handled elsewhere.
- Prescribing despite documented allergy: It is still not unusual for medicines to be prescribed even though the patient has a known allergy. Contributing factors include inconsistent documentation, failure to check allergy status, or failure to cross-check the ingredients of a medicine against allergy status before prescribing.¹⁰ These errors can lead to life-threatening anaphylaxis. Accurate, accessible, and routinely verified allergy information is essential for safe prescribing.⁶ ¹⁰
- Drug interactions: Drug interactions occur when two or more medicines are prescribed together without recognising that the combination may increase toxicity, reduce therapeutic effect, or destabilise a patient’s condition. Interactions involving medicines such as digoxin, antibiotics, anticoagulants, and antiepileptics are particularly high-risk.⁶ Effective patient screening with a thorough medication history and referring to up-to-date prescribing information are key to preventing these errors.⁶ ¹¹
Causes and risk factors
Prescribing errors can occur for many reasons. Research indicates that errors are seldom the result of a single factor, but rather arise from multiple pressures acting together. Contributing factors include: incomplete patient records, inadequate staffing, lack of knowledge, poorly designed systems, alert fatigue, and lack of collaboration.¹² Studies have associated higher error rates with a lack of prescribing training and distractions in the clinical environment⁶ ¹³ ¹⁴ which can make it more difficult for health professionals to concentrate and verify prescriptions. Evidence also points to the impact of poor communication, especially at clinical handovers and during admission, transfer, and discharge.
Prescribing errors are an ongoing challenge as the complexity of modern healthcare means that patients with multiple long-term conditions taking several medicines are at increased risk of experiencing problems due to drug interactions, contra-indications, and inappropriate dosing, particularly with high-risk drugs.⁶ ⁷ ¹⁴ ¹⁵
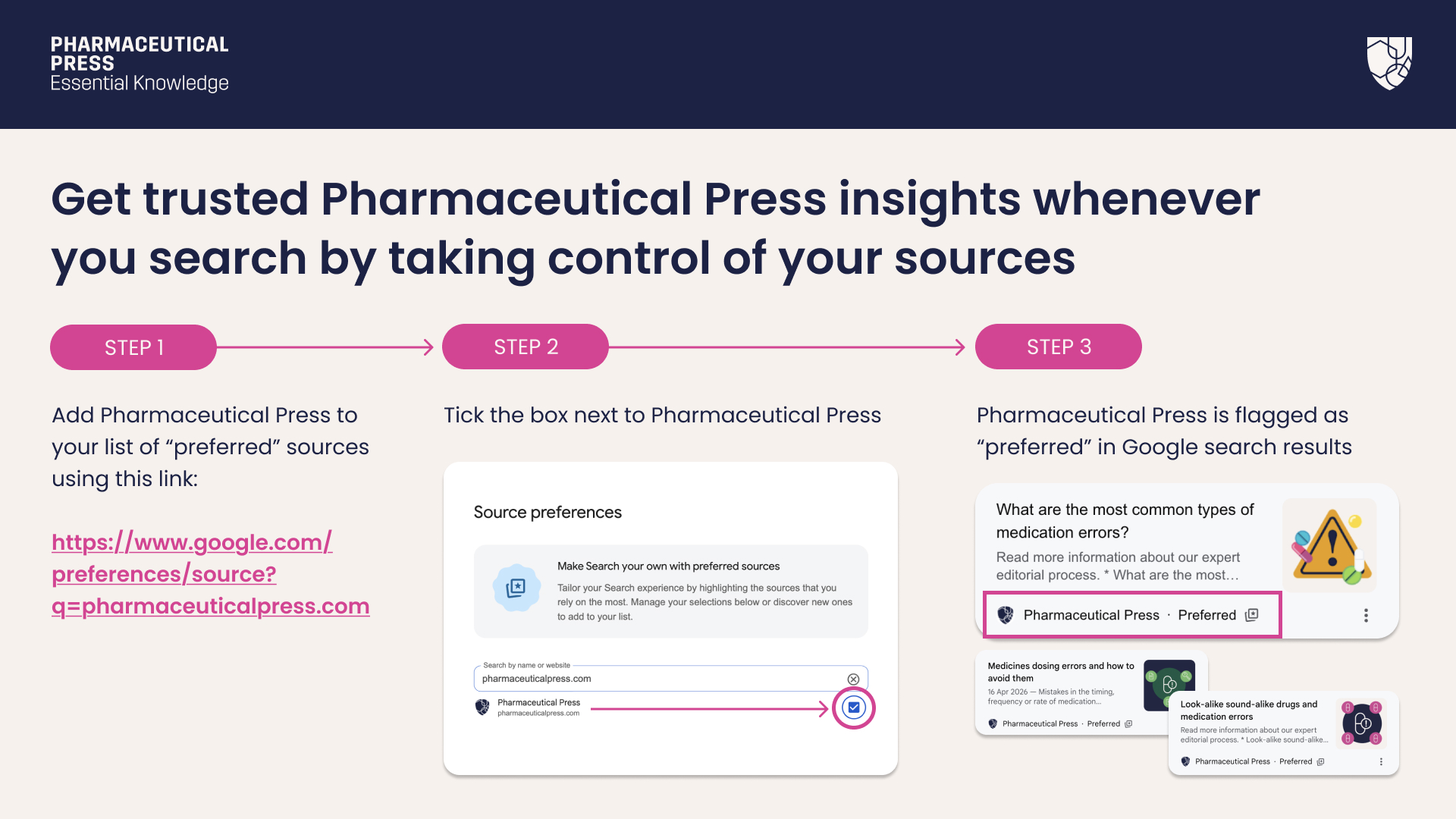
Add Pharmaceutical Press as a preferred source using this link. You must be logged in to Google to do so.
Prescribing errors in the UK and worldwide
Prescribing errors are a major cause of preventable harm worldwide, affecting all sectors of care.¹⁶ While patterns differ across healthcare systems, several consistent themes are evident. Issues such as communication breakdowns and workload pressures are consistently observed across settings. These shared challenges highlight the need for strong prescribing practices and systems and a culture of patient safety worldwide.
In the UK, prescribing errors are likely to be influenced by population needs and how care is delivered. The population continues to grow, with projections indicating it will reach 70 million by 2026. The proportion of people aged 65 or over was 19% in 2022, and this is expected to rise to 27% by 2072.¹⁷ An ageing population means more people will be living with several long-term conditions and taking multiple medicines so have a high risk of medication related harm.¹³ ¹⁷
In response, national priorities have shifted towards medicines optimisation, ensuring that prescriptions are both necessary and appropriate. Initiatives such as the NHS Patient Safety Strategy emphasise structured medication reviews and improved prescriber education, with the aim of reducing preventable harm and improving patient outcomes.
Preventing prescribing errors
Given the extremely high prevalence of these errors it is vital that a systematic approach is taken to prevent them.¹²
With so many contributing factors, multiple approaches to understand and mitigate the risks are required. System design improvements, electronic prescribing systems, and decision support tools can help reduce error rates.
Medication reviews are key to ensuring that all of a patient’s prescribed medicines and doses are appropriate and adjusted as required, for example, due to changes in organ function, and that the recommended therapeutic monitoring is in place. Medicines reconciliation at transitions of care is also important for continuity of essential medicines. Ongoing education for health professionals, structured induction programmes, and targeted training on high-risk medicines can help maintain safe prescribing standards.
The consistent use of reliable, evidence-based prescribing information including clinical guidelines is vital in reducing prescribing errors. Reference sources such as the BNF and BNFC provide essential support to health professionals in choosing appropriate medicines, determining correct doses, and identifying potential interactions or contra-indications.¹⁹
Prescribing errors remain a significant and preventable cause of harm in healthcare systems worldwide. Common errors include inappropriate choice of therapy, wrong doses, drug omissions, drug interactions, and failures in monitoring.⁶ ⁷ ⁸ Contributing factors include medicine factors, human factors, system pressures, and the increasing complexity of patient care.¹²
Improving prescribing safety requires a comprehensive approach, including better prescribing education, clear communication and collaboration within clinical teams, empowering patients, and robust medicines governance processes in all sectors of care. Digital health and artificial intelligence will also have an important future role to play in enhanced clinical decision making. By recognising common patterns of error and implementing practical safeguards, health professionals can reduce the risk of harm and improve patient outcomes.
Trial form
Please complete the form below to request a complimentary trial to knowledge products through MedicinesComplete.
References
- Elliott, R.A. et al.(2021) ‘Prevalence and economic burden of medication errors in the NHS in England’, BMJ Quality & Safety, 30(2), pp. 96–105. Available at: https://qualitysafety.bmj.com/content/30/2/96 (Accessed: 11 June 2026).
- Setra A. Workforce pressures and medication risk: time to act? The Pharmaceutical Journal, 04 June 2026 https://pharmaceutical-journal.com/article/opinion/workforce-pressures-and-medication-risk-time-to-act (Accessed: 11 June 2026).
- The NHS Patient Safety Strategy. NHS England. 2019. https://www.england.nhs.uk/patient-safety/the-nhs-patient-safety-strategy/.(Accessed: 11 June 2026).
- NHS Resolution (2023) Learning from medication errors. 30 March. Available at: https://resolution.nhs.uk/2023/03/30/learning-from-medication-errors/ (Accessed: 15 May 2026).
- Aronson, Jeffrey K. “Medication errors: definitions and classification’. British Journal of Clinical Pharmacology, vol. 67, no. 6, June 2009, pp. 599–604. PubMed, https://doi.org/10.1111/j.1365-2125.2009.03415.x.
- Cousins, David, et al. ‘Thetopten prescribing errors in practice and how to avoid them’. The Pharmaceutical Journal, 21 Feb. 2019, https://pharmaceutical-journal.com/article/ld/the-top-ten-prescribing-errors-in-practice-and-how-to-avoid-them (Accessed: 11 June 2026).
- Coon R. High-risk medications: a guide for pharmacy professionals. The Pharmaceutical Journal, 5 September 2025 High-risk medications: a guide for pharmacy professionals – The Pharmaceutical Journal (Accessed: 11 June 2026).
- Willis S. Are electronic prescribing systems increasing the risk of ‘look-alike sound-alike’ medication errors? The Pharmaceutical Journal, (Accessed: 11 June 2026).
- Basey AJ, Krska J, Kennedy TD, Mackridge, Prescribing errors on admission to hospital and their potential impact: a mixed-methods study. BMJ Qual Saf. 2014 Jan;23(1):17-25
- NHS Resolution Anti-infective medication errors. Anti-infective medication errors – NHS Resolution. Available at: https://resolution.nhs.uk/resources/anti-infective-medication-errors/ 16 August 2022 (Accessed: 12 June 2026).
- Drug interactions: resources to support clinical decisions – NHS SPS – Specialist Pharmacy Service – The first stop for professional medicines advice. Available at: https://www.sps.nhs.uk/articles/drug-interactions-resources-to-support-clinical-decisions/ (Accessed: 13 June 2026).
- Preventing errors on the medicine journey – NHS SPS – Specialist Pharmacy Service – The first stop for professional medicines advice. Available at: https://www.sps.nhs.uk/articles/preventing-errors-on-the-medicine-journey/ (Accessed: 13 June 2026).
- Avery T, Barber N, Ghaleb M et al. Investigating the prevalence and causes of prescribing errors in general practice. Available at: https://www.gmc-uk.org/about/what-we-do-and-why/data-and-research/research-and-insight-archive/investigating-the-prevalence-and-causes-of-prescribing-errors-in-general-practice (Accessed: 20 May 2026).
- Walker, L. E. &Pirmohamed, M. (2023). Increasing trend in hospitalisation due to adverse drug reactions: can we stem the tide? Drug & Therapeutics Bulletin, 61 (6), 87-91. https://dx.doi.org/10.1136/dtb.2022.000050
- Accessing resources for patients on high risk medicines’. SPS – Specialist Pharmacy Service, 19 Dec. 2022. Available at: https://www.sps.nhs.uk/articles/accessing-resources-for-patients-on-high-risk-medicines/ (Accessed: 11 June 2026).
- Global Burden of Preventable Medication-Related Harm in Health Care: A Systematic Review. Availaible at: https://www.who.int/publications/i/item/9789240088887 (Accessed: 15 June 2026).
- House of Commons Library (2024)The UK’s changing population. 16 July. Available at: https://commonslibrary.parliament.uk/the-uks-changing-population/ (Accessed: 20 May 2026).
- Ageing and Health. Available at: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health. (Accessed 21 May 2026).
- BNF + BNFC. Available at: https://www.medicinescomplete.com/ (Accessed: 21 May 2026).


