ADHD medication
Attention deficit hyperactivity disorder (ADHD) has become a widely discussed medical condition in the media. Many will have a direct or indirect connection to the condition, whether through family members, friends, or personal experience.
Yet despite increased awareness, negative perceptions of ADHD remain prevalent. Social stigma can be damaging, contributing to reduced self-esteem and discouraging individuals, particularly adults, from seeking diagnosis and appropriate support.
At the same time, social media has contributed to a shift in how ADHD is discussed, with greater emphasis on recognising individual challenges and supporting effective management. As more people share their experiences, awareness and understanding of the condition have improved. However, negative stereotypes persist and continue to influence attitudes.
With rising referrals and diagnoses, it is increasingly important that health professionals are well equipped to manage and support individuals with ADHD. A clear, evidence-based understanding of ADHD and its management is essential to ensure appropriate and effective long-term care.
Please complete the form at the bottom of this article to request a complimentary trial of MedicinesComplete.
Overview of ADHD
ADHD is a common neurodevelopmental disorder; it has a chronic course with symptoms that begin in early childhood but often persist into adult life.¹ ²
Symptoms may be overlooked in earlier years, so that people go untreated. The condition often leads to impaired functioning across multiple settings, such as home, education, employment and relationships.
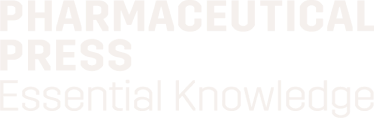
The prevalence of ADHD varies significantly worldwide due to variable diagnostic practices and how rigorously the criterion for impairment is applied¹ . The UK prevalence in adults is estimated at 3% to 4%² and in children the global prevalence is estimated at around 5%³. In February 2026, it was estimated that around 2.5 million people in England have ADHD⁴, a figure which includes individuals who may remain undiagnosed. Of these an estimated 741,000 are children and young people (aged 5-24).
The core ADHD symptoms are;¹ ² ³ ⁵ ⁶
- Inattention: for example, difficulty with attention and maintaining focus, following instructions or engaging in tasks that require sustained mental effort.
- Hyperactivity: for example, persistent restlessness, fidgeting, running about inappropriately or talking excessively.
- Impulsivity: for example, saying or doing things without consideration of consequences, interrupting or intruding on others or behaving recklessly.
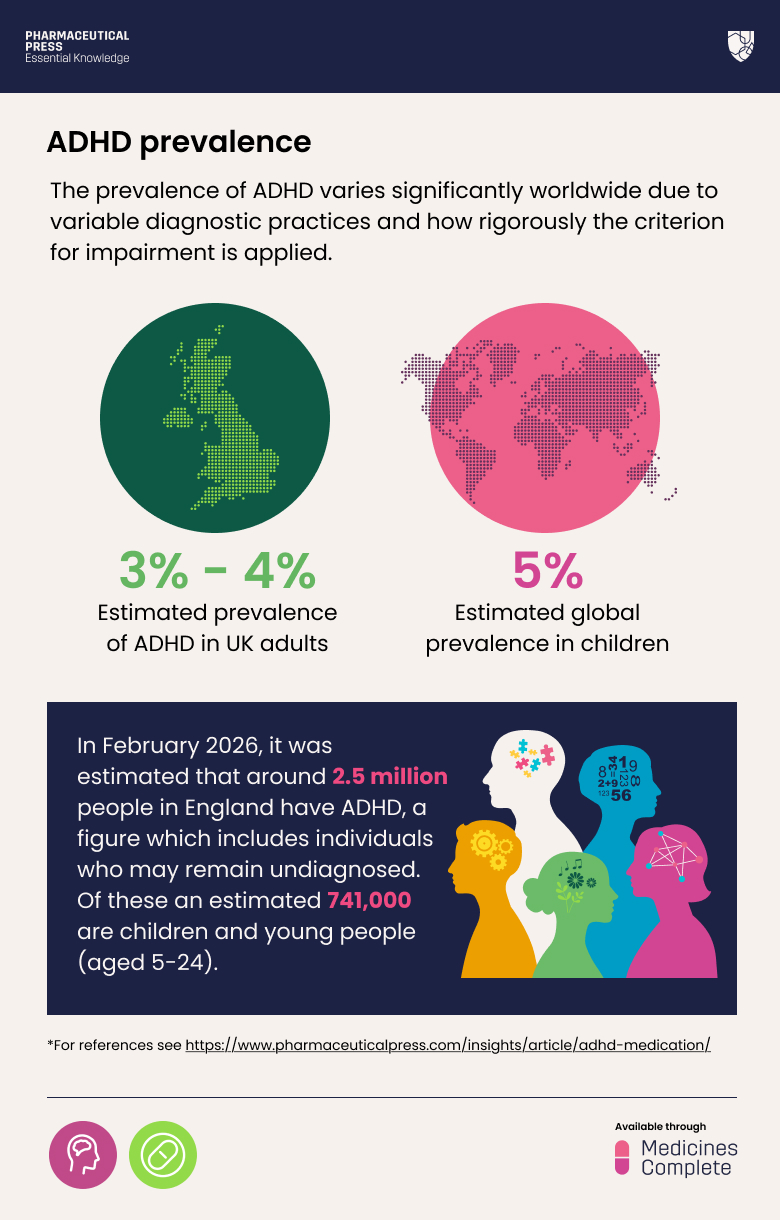
Add Pharmaceutical Press as a preferred source on Google using this link. You must be logged in to Google to do so.
Not everyone diagnosed will have all three symptoms. The symptoms generally emerge in childhood, usually before the age of 12 years, and their presentation varies with gender and changes with age⁹. For example, hyperactivity in adults often presents as feelings of inner restlessness and agitation, rather than overt hyperactivity.² Adults also frequently report excessive mind wandering and difficulty regulating emotions.
A high proportion of both children and adults with ADHD will have one or more co-morbidities, such as autism spectrum disorder, mood disorders, and personality disorders. Most children will continue to experience symptoms into adolescence and up to 60% will do so into adulthood.¹ ²
ADHD in children and young people affects many areas of life, including school, family relationships, friendships, activities, and self-esteem.³ In later life, it can contribute towards difficulties such as underachievement at work, relationship problems, and self-harm.²
ADHD can affect not only the individual but also have a significant impact on families and communities. Parents, in particular, may be unfairly blamed for a child’s behavioural issues. The wider impact of ADHD requires health professionals to take a holistic management approach.
Managing ADHD
The management of ADHD requires a multi-faceted approach to address psychological, behavioural, occupational and educational needs.⁸ Diagnosis is undertaken by psychiatrists, paediatricians and other specialists with expertise in ADHD.¹ ³ There should be a written treatment plan shared between health professionals and the person with ADHD; for children, this may be shared more widely (for example, with families, schools or social care, if relevant and agreed).⁸
Both pharmacological and non-drug interventions are used with the aim of controlling symptoms and improving quality of life.⁷ Guidelines from the National Institute for Health and Care Excellence (NICE) outline the general treatment approach, highlighting that people with ADHD, and their family members or carers, should be involved in treatment planning and decisions.⁸
Drug treatments should only be a part of the overall treatment plan. In the UK, a ‘watchful waiting’ approach is recommended initially in children with psychoeducation and behavioural therapy, before moving on to drug treatment.³ A similar approach is taken in adults, although medication is usually the first-line option.² ⁸
- Pharmacological management
The medicines used in ADHD modulate neurotransmitters, such as dopamine and noradrenaline, in the area of the brain that regulates attention, behaviour and emotion.⁹ Stimulant and non-stimulant medicines are used; there are important differences between them that determine how they are prescribed and used. Stimulants are short acting and start to work quickly whereas non-stimulants can take several weeks to start working.⁹
- Stimulant medicines
Stimulant medicines are the recommended first-line pharmacological therapy for ADHD across all age groups (except children under five years old). Medication should only be initiated by a health professional with training and expertise in diagnosing and managing ADHD. In pre-school age children under five years medication should only be prescribed on the advice of two specialists due to limited evidence on efficacy and safety.⁸ Stimulant medicines are either methylphenidate-based or amphetamine-based (lisdexamfetamine and dexamfetamine in the UK).² ³ ⁸ Lisdexamfetamine or methylphenidate are the first-line drug options. Dexamfetamine is used less often as there is more limited evidence on efficacy and safety. Stimulant medications are Schedule 2 controlled drugs and must be prescribed in line with the Misuse of Drug Regulations.
Methylphenidate has a large evidence base and is usually the first-line option in children when a drug is indicated.¹⁰ The decision to prescribe it should include consideration of co‐morbidities, tolerability and adverse effects, convenience of dosing, the potential for misuse and patient/parent preference. Adverse effects include insomnia, anorexia, raised blood pressure and growth deceleration – which can usually be managed by symptomatic management and/or dose reduction.⁸ ¹²
Lisdexamfetamine itself is pharmacologically inactive, but acts as a pro-drug of dexamfetamine.¹⁰
A prodrug can be defined as a molecule, which on its own does not have any biological activity, however through a serious of biological processes, including its own metabolism it is able to generate a biologically active drug.¹¹ Lisdexamfetamine is dexamfetamine complexed with lysine. After oral administration it is quickly absorbed from the gastrointestinal tract and then converted (mainly within red blood cells) into dexamfetamine.¹¹ Dexamfetamine is the active form responsible for the pharmacological effects of lisdexamfetamine.
Stimulants may not be appropriate for patients with cardiovascular disease, moderate to severe hypertension, hyperthyroidism, or psychosis, as they can worsen these conditions.¹²
Psychotropic Drug Directory, available via MedicinesComplete, provides health professionals with rapidly accessible information, advice and references on psychiatric drugs. Chapter three supports optimal medicine choice in people with co-morbidities including cardiovascular disease, diabetes and hepatic and renal impairment.
- Stimulant medicines – formulation issues
There is a wide range of preparations of methylphenidate with different release profiles.⁷ ⁹ Modified-release (MR) preparations of stimulants are preferred because of their pharmacokinetic profile, convenience, improved adherence, reduced risk of drug diversion (i.e. drugs being forwarded to others or misused), and no requirement to be taken to work or school.¹³ Immediate-release preparations can be given during dose titration or when more flexible dosing regimens are required. Taking a combination of immediate and modified release preparations at different times of the day can be used to extend the duration of effect.
Methylphenidate MR products should be prescribed by brand, as different formulations contain varying proportions of immediate and modified-release components.⁹ ¹⁴ These differences can affect the release and absorption of the drug, and products may not be clinically equivalent. Prescribing by brand, or specifying the manufacturer alongside the generic name, helps to maintain consistency in therapeutic effect and supports patient safety.
Switching between brands should only be done in essential situations, such as during supply disruptions, and caution is needed due to the potential impact on symptom control. Decisions regarding product choice should be individualised, involve specialist input, and be made in partnership with the patient. Patients should be counselled about any potential changes, and health professionals should provide reassurance where appropriate. If a switch is required, it should be temporary, and mixing brands to achieve doses should be avoided. Patients should be returned to their usual branded product as soon as supply allows.¹⁴
Patients receiving stimulant medications for ADHD require regular monitoring to assess clinical effectiveness and to detect potential adverse effects. In children, monitoring is especially important as some ADHD medications can affect growth and development. Ongoing review should be tailored to the individual, considering both the severity of ADHD and current treatment status.³ ⁸ ⁹
- Non-stimulant medicines
Some patients may not respond to stimulant medications, or they may be unsuitable due to contraindications, side effects or potential drug interactions. In such cases, specialists may decide to manage ADHD symptoms using non-stimulant medications. The most commonly used nonstimulants are atomoxetine and guanfacine.
Atomoxetine works by blocking the reuptake of noradrenaline in the brain. It has little effect on serotonin or dopamine and minimal interaction with other neurotransmitter receptors. It is less effective than stimulants.¹⁰ It may be particularly useful for children who do not respond to stimulants, where stimulant diversion is a problem or when ‘dopaminergic’ adverse effects (such as tics) become problematic on stimulants.³
Parents should be warned of the possibilities of suicidal thinking and liver disease emerging and advised of the possible features they might notice.
Guanfacine is another non-stimulant medication; it is a selective α2A-adrenergic receptor agonist. Although its exact mechanism of action in ADHD is not fully understood, it is thought to improve synaptic transmission in brain regions such as the prefrontal cortex.⁹ It is unlicensed for use in adults. Gaunfacine is a third-line treatment option in children and young people, used when other treatments are not suitable.³
Non-pharmacological interventions
The current best practice approach to ADHD treatment combines medication with behavioural therapies and environmental support tailored to the individual’s needs.² ³ ⁸ ¹⁵ ¹⁶
Non-pharmacological intervention is an umbrella term that covers any treatment other than medication, including parent training, psychoeducation, talking therapies, and cognitive behavioural therapy (CBT). Non-pharmacological interventions have an important role in managing ADHD symptoms, particularly in children.¹⁶ Patients should be encouraged to use these strategies alongside standard therapy. In adults, these approaches may be considered for those who: choose not to have medication, who find it difficult to adhere to medication, or who have found medication to be ineffective or not tolerated.
Regular exercise and a balanced diet are widely recognised as positive lifestyle choices.⁸ Insomnia and lack of adequate sleep are common symptoms of ADHD. Patients are encouraged to practice good sleep hygiene, such as warm baths and avoiding use of stimulating devices before bed, and reducing caffeine and alcohol intake.
Case study
Patient A is a 42 year-old male with a recent diagnosis of ADHD. He was initiated on methylphenidate by a consultant psychiatrist eight weeks ago, and the dose has been titrated gradually to 60mg daily (20mg three times a day). He presents to his GP complaining of feeling anxious and he has noticed occasional heart palpitations. The patient also has asthma, which is well controlled with a combination inhaler of formoterol and beclomethasone, and a history of anxiety, although he is not currently taking any medicines for this. On examination, the patient has tachycardia (120 bpm) and elevated blood pressure (145/95 mmHg).
Methylphenidate is a specialist medicine, and the GP is aware from the patient’s record that there was no evidence of any cardiovascular problems on the examinations required before methylphenidate was started. The GP consults Martindale’s ADR Checker as he is aware there are some important cardiac side effects with methylphenidate. Palpitations, hypertension and anxiety are all noted as common side effects with methylphenidate.¹⁷ In the management section, it states that if the potentially causative drug is needed, it is recommended to use the lowest effective dose as blood pressure elevations are often dose-dependent.
The GP recognises that these symptoms may mean methylphenidate needs to be stopped. The patient also has a history of anxiety, however, and some of his symptoms are also a feature of this condition. In light of this, the GP decides to proceed cautiously and to liaise promptly with the patient’s specialist and ADHD clinic to discuss the best course of action.
The specialist recommends that the methylphenidate dose is reduced to 30mg daily in the meantime and she will arrange an appointment at the clinic for further assessment as soon as possible.
This approach ensures:
- Coordinated care between primary and secondary care services.
- Agreement on ongoing ADHD treatment.
- Consideration of whether methylphenidate needs to be stopped and switched to an alternative ADHD treatment.
- Ensuring appropriate monitoring (e.g. regular BP and pulse checks) and follow up.
For many individuals, an ADHD diagnosis is not always straightforward and may present challenges, including navigating social stigma and concerns about how they are perceived by others. ADHD is a lifelong condition, and although symptoms vary between individuals, untreated or poorly managed ADHD is associated with reduced quality of life and poorer health and social outcomes, highlighting the importance of effective and timely intervention.
Health professionals have an important role in the appropriate and holistic management of ADHD. Effective management involves ensuring that patients are on the most appropriate treatment for their individual needs, and that decision-making is shared with the patient and/or carers.² ³ ⁸
Trial form
Please complete the form below to request a complimentary trial to knowledge products through MedicinesComplete.
References
- Johal M and Haria D, Attention deficit hyperactivity disorder: characteristics and diagnosis, The Pharmaceutical Journal, 11 April 2023. Available at: https://pharmaceutical-journal.com/article/ld/attention-deficit-hyperactivity-disorder-characteristics-and-diagnosis (Accessed: 2 July 2026).
- Attention deficit hyperactivity disorder in adults – Symptoms, diagnosis and treatment | BMJ Best Practice. Available at: https://bestpractice-bmj-com.knowledge.idm.oclc.org/topics/en-gb/814 (Accessed: 2 July 2026).
- Attention deficit hyperactivity disorder in children | BMJ Best Practice. Available at: https://bestpractice-bmj-com.knowledge.idm.oclc.org/topics/en-gb/142/epidemiology (Accessed: 2 July 2026).
- NHS Digital (2026) Mental Health of Children and Young People in England 2026: ADHD data (MI ADHD), February 2026. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/mi-adhd/february-2026 (Accessed: 2 June 2026).
- ADHD in Children and Young People. rcpsych.ac.uk. Available at: https://www.rcpsych.ac.uk/mental-health/parents-and-young-people/information-for-parents-and-carers/ADHD-in-young-people (Accessed 2 June 2026).
- ADHD in Adults. rcpsych.ac.uk. Available at: https://www.rcpsych.ac.uk/mental-health/mental-illnesses-and-mental-health-problems/adhd-in-adults (Accessed 29 June 2026).
- Johal M and Haria D, Attention deficit hyperactivity disorder: management and support, The Pharmaceutical Journal, 18 April 2023. Available at: https://pharmaceutical-journal.com/article/ld/attention-deficit-hyperactivity-disorder-management-and-support (Accessed 29 June 2026).
- Recommendations | Attention Deficit Hyperactivity Disorder: Diagnosis and Management | Guidance | NICE. 14 March 2018. Available at: https://www.nice.org.uk/guidance/ng87/chapter/recommendations#maintenance-and-monitoring (Accessed: 2 July 2026).
- Mansoorali K., Stimulant and non-stimulant agents for ADHD, The Pharmaceutical Journal, 11 April 2025. Available at: https://pharmaceutical-journal.com/article/ld/stimulant-and-non-stimulant-agents-for-adhd (Accessed: 2 July 2026).
- Taylor DM, Barnes, RE and Young, AH. The Maudsley Prescribing Guidelines in Psychiatry 13th Edition, 2018. P496 – 504.
- ScienceDirect (n.d.) Prodrug. Available at: https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/prodrug (Accessed: 26 June 2026).
- Attention deficit hyperactivity disorder | Health topics A to Z | CKS | NICE. Available at: https://cks.nice.org.uk/topics/attention-deficit-hyperactivity-disorder/ (Accessed: 3 July 2026).
- Treatment summary: Attention deficit hyperactivity disorder, BNF, MedicinesComplete. Available at: https://www.medicinescomplete.com/ (Accessed: 3 July 2026).
- ‘Prescribing and Switching between Modified-Release Methylphenidate’. SPS – Specialist Pharmacy Service, 16 Nov. 2023. Available at: https://www.sps.nhs.uk/articles/prescribing-and-switching-between-modified-release-methylphenidate/ (Accessed: 30 June 2026).
- Sibley M, Bruton A, Zhao X et al. Non-pharmacological interventions for attention-deficit hyperactivity disorder in children and adolescents. The Lancet Child & Adolescent Health, 2023; 7, 415-428.
- Sibley, M. H., Flores, S., Murphy, M., et al. Research Review: Pharmacological and non-pharmacological treatments for adolescents with attention deficit/hyperactivity disorder – a systematic review of the literature. Journal of Child Psychology and Psychiatry. 2025;66(1):132-149. doi:10.1111/jcpp.14056
- Available at: https://www.medicinescomplete.com/ (Accessed: 3 July 2026).